

Ali et al. reported in 1991 that natural honey had an inhibitory effect on Helicobacter pylori in vitro, at solutions of both 10% and 20% honey, and proposed that clinical studies on the treatment of H. pylori infection be undertaken[5]. Al Somal et al. performed in vitro experiments to determine what concentrations of honey would be inhibitory for H. pylori, what the active component of the honey is, and whether it was merely an osmotic effect that inhibits H. pylori. They found that Manuka honey from New Zealand, at concentrations as low as 5% v/v, completely inhibit the growth of H. pylori, and that 2.5% v/v partially inhibits the growth of H. pylori. The authors also found that non-Manuka honey, and an artificially prepared solution mimicking the physical properties of honey, had no inhibitory effect on H. pylori. The authors stated that although the active property in Manuka honey has not been identified, they know it is a hydrophilic molecule of a weight of 500 Daltons that is stable at a pH of 1. They proposed clinical trials, and the possibility that an extract of the Manuka tree or Manuka honey could be used in the eradication of H. pylori[6]. Although no such large-scale trial has been undertaken, McGovern et al. reported on a small series of volunteers with Helicobacter pylori infection by 14C urea breath tests, treated with Manuka honey or Manuka honey and omeprazole. After two weeks of treatment, all 12 of the patients remained positive for H. pylori by 14C urea breath test. The authors concluded that, if Manuka honey is effective against dyspepsia, it is not due to eradication of H. pylori[9].
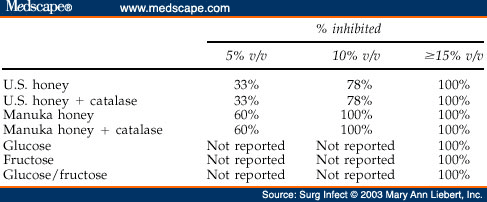
Osato et al. revisited the topic in 1999; they compared Manuka honey to honeys obtained commercially from Texas and Iowa, and to an artificially prepared solution mimicking honey ( ). They found that at concentrations .15% v/v, all honeys and the artificial solution inhibited growth of all H. pylori isolates tested. Additionally, when catalase was added to the honeys concentrated .15% v/v, the honeys retained their ability to inhibit all H. pylori isolates; therefore, the anti-Helicobacter pylori activity was interpreted to be due to the osmotic effect, as opposed to hydrogen peroxide content. At the lowest concentration tested, 5% v/v, the Manuka honey inhibited 60% of the isolates tested, whereas the U.S. honeys inhibited only 33% of the Helicobacter pylori isolates tested. This difference was not statistically significant. The authors concluded that non-oxidant effects are important in bacterial killing, and that paramount among these effects is the osmotic effect. They also concluded that since 15% v/v honey was needed to inhibit all Helicobacter pylori, that honey would not be a feasible treatment for Helicobacter pylori, as it would probably not be possible to maintain this concentration at the gastric mucosa[7]. In fairness, they probably should have concluded that the Manuka honey deserved further investigation for its non-oxidant, non-osmotic killing property, due to the intriguing, if not statistically significant finding of differences in H. pylori inhibition at 5% v/v concentrations.
Table 2. H. Pylori Isolates Inhibited by Various Solutions, After Osato et al.[7]
Finally, Booth suggested in a letter to the editor that if there is so much interest in the role of honey eradicating Helicobacter pylori, and Helicobacter pylori has been postulated to have a role in the pathogenesis of gastric lymphoma, that there should be interest in the use of honey as a possible cure for a form of gastric cancer[8].
more information:
https://www.medscape.com/viewarticle/458834_7